Monday, October 31, 2016
Can Depression Be Cured with a Vitamin? B12
Cure Depression with a Vitamin?
Have you ever wondered if depression could be eased with an inexpensive over-the-counter supplement, no prescription required? Or how about extinguishing your chronic anxiety through more consumption of certain foods that contain natural stress-reducing ingredients? Read on, because I’ve got something for you that will both surprise and delight.
Every day I see patients who want to do everything in their power to avoid mind-altering pharmaceutical drugs. This is especially true of women hoping to become pregnant or who already are. Among the tests I order to get a sense of my patients’ biology when they first come see me, one of the results I like to review immediately is their level of vitamin B12. Is it low? If so, could it be the reason they are in my office to begin with?
Vitamin B12 deficiency has long been implicated in the development of depression.
It’s one of the basic building blocks of life. And it’s one of the all-star antidepressants. We all need vitamin B12 to make red blood cells and nerve cell membranes and to regulate the expression of our DNA and multiple other brain and body-based functions. It protects the brain and nervous system, regulates rest and mood cycles, and keeps the immune system functioning properly. A severe deficiency can lead not only to deep depression, paranoia and delusions, and memory loss, but also incontinence, the loss of taste and smell, and, eventually, physical brain shrinkage and dementia. The medical literature is filled with case reports of people with these conditions that a single shot of vitamin B12 cured. In fact, one of my favorite game-changing papers was a 2003 case report of a lifelong vegetarian who experienced a month and half of progressively worsening depression. Eventually she began to hear voices and feel paranoid. The fifty-two-year-old postmenopausal woman ultimately became what’s called catatonic, which meant she was awake and alive but nonresponsive, and largely in an otherwise vegetative state. You would automatically assume this was a serious case of severe pathology, right? She was treated with electroconvulsive therapy and antipsychotics to no avail. And then she was transferred to another hospital, where they happened to test her levels of vitamin B12. Guess what: That’s when they discovered she was a tad on the low side, and after receiving a vitamin B12 injection, she fully recovered. She was back to her old self quickly—her healthy self from 14 years previously—and needed no more treatment. While it may be one of the more extreme cases, it’s emblematic of how a simple but critical deficiency can be at the casual root of psychiatric manifestations and subsequent high-risk interventions.
Some two-fifths of the population is severely deficient in B12 for a variety of reasons, from poor diet and dysbiosis (a disrupted gut flora) to use of medications like acid-reflux (e.g., Prilosec and Nexium, what are referred to as “proton-pump inhibitors”) and diabetes drugs. Vegans and vegetarians may have to extra cautious about becoming deficient because the richest source of vitamin B12 is found in animal products such as fish, poultry, meat, and eggs (hence the case of the lifelong vegetarian—it eventually caught up with her).
It’s standard in my practice to order a simple blood test to determine B12 levels in patients. It’s practically a no-brainer for me today, as I know I can meaningfully move the health needle for many patients with this simple intervention. (Deficiency is traditionally defined as being below 150 to 200 pg/mL (picogram/milliliter), but you want to be above 600 pg/mL for optimal health.) I am especially vigilant about pregnant women, for babies born to a mother deficient in B12 are at serious risk for neurological symptoms such as lethargy, developmental delays, and delayed cognitive and motor development.
So you must ask yourself: Is your depression being fueled by low B12? Could you cure your depression and get on with you life via a B12 supplement that costs as much as a ticket to a movie for a month supply?
Tip: Vitamin B12 comes in a few different forms, which vary in efficacy and safety. Cyanocobalamin is the most commonly used form of the nutrient. It’s less expensive, but it is not found in nature, and its metabolism may release small amounts of cyanide into the system. That’s right: cyanide. While this could never be enough to cause cyanide poisoning, it’s a potential issue for people who have impaired detox as a result of genetic issues, nutrient deficiencies, or chronic illness. The most desirable form of B12 is methylcobalamin, which is the form found produced by our gut bacteria. So when you’re looking for a B complex, make sure it contains B12 as methylcobalamin (or hydroxocobalamin or adenosylcobalamin) in addition to the other B vitamins.
Extra Tip: When you get your vitamin B12 levels checked, also have your homocysteine levels checked too. This is a more accurate and more sensitive method of screening for vitamin B12 deficiency. Homocysteine is a potentially inflammatory protein that must be metabolized by B12 and folate. Optimal levels of homocysteine are between 7 and 10 micromoles per liter of blood. Typically a homocysteine over 8 is a red flag for inflammation that may be responsive to B12 supplementation.
This is one of many ways in which depression (and fatigue, and brain fog, etc.) presents an invitation to recalibrate, rebalance, and reexamine ways in which to better support our bodily organism.
139
Share
Tweet
1
Share
3
Share
Filed Under: Anxiety, Defeat Depression, Depression, Hormones, Pregnancy and Mood, Rethink Health, Sane Motherhood, Self Improvement, Stress
Tagged With: Chronic Fatigue, Cyanocobalamin, Dementia, Vegetarians, Vitamin B12, Vitamin Deficiency
Sunday, October 30, 2016
Allergens in Vaccines Are Causing Life-Threatening Food Allergies
Allergens in Vaccines Are Causing Life-Threatening Food Allergies: Why have life-threatening food allergies become so alarmingly pervasive? #featured_mcat_vaccination
√Red Light Therapy Benefits, Research & Mechanism of Action
Red Light Therapy Benefits, Research & Mechanism of Action
Dr Josh Axe
Through emitting red, low-light wavelengths through the skin, red light therapy helps naturally jump-start the process of tissue recovery and other forms of rejuvenation through increased blood flow, collagen stimulation and more. 2010 marked the 50th anniversary for medical laser treatments like red light therapy, providing a host of evidence on their benefits. (1)
If you’ve never heard of red light therapy before, you might already be familiar with other terms that are used to describe this treatment, such as low level laser therapy (LLLT), biostimulation (BIOS), photonic stimulation or simply light box therapy. Red light is considered “low level” because it works at an energy density that’s low compared to other forms of laser therapies.
Red light therapies have come a long way, but do they really work? Clinical studies show that, yes, red lightbox therapies have certain healing capabilities and medical applications thanks to the way they positively affect the human endocrine and immune systems. LLLT is now FDA-approved for treating conditions like chronic joint pain and slow-to-heal wounds. In the near future, we can expect approval for many more conditions thanks to red light benefits, such as increased immunity, tissue repair, anti-aging effects, improved joints and more.
What Is Red Light Therapy?
Red light therapy involves having low-power red light wavelengths emitted directly through the skin, although this process cannot be felt and isn’t painful because it doesn’t produce any heat. Red light can be absorbed into the skin to a depth of about eight to 10 millimeters, at which point it has positive effects on cellular energy and multiple nervous system and metabolic processes.
Red light therapy has shown promise for treating symptoms of joint pain or osteoarthritis due to aging, those caused by cancer treatments like chemotherapy or radiation, hair loss, wounds or incisions, acne, wrinkles and skin discoloration, chronic muscular pain, neurological damage, and tissue damage (often at the root of tears, sprains or pulls). As you’ll learn, even seeing the color red is physically stimulating, primes our senses and gets our blood pumping, so imagine what red light penetrating right into your body can do.
Although there is still controversy over this treatment and more research needed, according to the company Light Therapy Options LLC, there are virtually “no known adverse side effects” of red light therapy treatments, rather a growing list of many anti-aging benefits. (2)
Some of the ways that red light wavelengths work are: (3)
- Increasing energy levels by promoting release of ATP from cells’ mitochondria (4)
- Stimulating DNA/RNA synthesis (5)
- Activating the lymphatic system, an important part of our immune system that helps carry waste out of the body
- Increasing blood flow/circulation, thereby helping bring more oxygen and nutrients to our cells and tissues
- Forming new capillaries (small blood vessels)
- Improving natural production of collagen and fibroblasts, important for things like skin, joint and digestive health
- Repairing and restoring damaged soft connective tissue
- Stimulating or decreasing inflammation, which helps control our natural healing capabilities
- Lowering effects of oxidative stress/free radical damage, which is associated with many effects of aging
5 Benefits of Red Light Therapy
1. Increased Immunity and Reduced Side Effects of Cancer Treatments
Research done by NASA in conjunction with the University of Alabama at Birmingham Hospital has shown that red light technology can successfully reduce symptoms experienced by cancer patients, including painful side effects caused from radiation or chemotherapy. Using far red/near-infrared light-emitting diode devices (called High Emissivity Aluminiferous Luminescent Substrate, or HEALS in this case) has been shown to release long wavelength energy in the form of photons that stimulate cells to aid in healing.
NASA tested whether HEALS could treat oral mucositis in cancer patients, a very common and painful side effect of chemotherapy and radiation, and concluded that 96 percent of patients experienced improvement in pain as a result of the HEALS treatment. Patients received the light therapy by a nurse holding the WARP 75 device, which is roughly the size of an adult human hand. The WARP device was held close to the patient’s face and neck for only 88 seconds daily for 14 days. Researchers stated, “The HEALS device was well tolerated with no adverse affects to bone marrow and stem cell transplant patients….The HEALS device can provide a cost-effective therapy since the device itself is less expensive than one day at the hospital.” (6)
Similar HEALS technology is also now being utilized for the treatment of pediatric brain tumors, slow-healing wounds or infections, diabetic skin ulcers, and serious burns.
2. Wound Healing and Tissue Repair
Light in the spectral range of 600 to 1,300 nanometers has been found to be useful for promoting wound healing, tissue repair and skin rejuvenation, although it does this through a different mechanism of action compared to many other laser resurfacing treatments. Most laser therapies used in dermatology offices use intense pulsed light to promote skin rejuvenation by inducing secondary tissue repair. In other words, they cause intentional damage to either the epidermis or the dermis of the skin in order to trigger inflammation, followed by healing.
Red light therapy actually bypasses this initial destructive step and instead directly stimulates regenerative processes in the skin through increased cellular proliferation, migration and adhesion. Red light therapy has been shown to positively affect skin cells through regeneration of fibroblasts, keratinocytes and modulation of immune cells (including mast cells, neutrophils and macrophages) all found within skin tissue.
3. Anti-Aging Effects for Skin and Hair Loss
One use of red light laser therapy that’s growing in popularity is reversing signs of aging on the skin (i.e, wrinkles and fine lines). Results from a 2014 study published in Photomedicine and Laser Surgery demonstrated both efficacy and safety for red light therapy in promoting anti-aging skin rejuvenation and intradermal collagen increase when compared against controls. (7) Researchers concluded that red infrared therapy “provides a safe, non-ablative, non-thermal, atraumatic photobiomodulation treatment of skin tissue with high patient satisfaction rates.”
Subjects treated with red light therapy experienced significantly improved skin complexion, improved skin tone, improved texture/feeling, reduced skin roughness, reduced signs of wrinkles and fine lines, and increased collagen density as measured through ultrasonographic tests. Patients with rosacea and redness have also found relief using LLLT, even those who are unable to tolerate higher-heat laser therapies.
Yet another anti-aging effect of red light therapy is reversing hair loss and stimulating follicle growth, which works in many of the same ways as red light therapy for wound healing. Results have been mixed according to studies, but at least a moderate portion of both male and female patients have had positive results for reversing baldness/hair loss when using LLLT. (8)
4. Improved Joint and Musculoskeletal Health
Red light therapy is now being used to treat arthritis symptoms thanks to its capability of stimulating collagen production and rebuilding cartilage. A 2009 Cochrane review of red light therapy for rheumatoid arthritis concluded that “LLLT could be considered for short-term treatment for relief of pain and morning stiffness for RA patients, particularly since it has few side-effects.” (9)
Even in those who don’t suffer from arthritis but have other signs of tissue damage or degeneration due to aging, LLLT can still be beneficial. A 2009 study published in The Lancet showed, “LLLT reduces pain immediately after treatment in acute neck pain and up to 22 weeks after completion of treatment in patients with chronic neck pain.” (10) Other studies have found that even when patients with musculoskeletal disorders don’t experience less pain from red light therapy treatments, they have a high chance of experiencing “significantly improved functional outcomes,” such as better range of motion. (11)
Cellular rejuvenation and increased blood flow due to red light therapy are two key aspects of improving joint and tissue health. Decreasing oxidative damage, which degenerates joints, and modulating inflammation are other ways that LLLT benefits soft/connective tissue.
5. Reduced Depression and Fatigue
Another way to explain the benefits of red light is through the lens of Eastern medicine. Ask a Traditional Chinese Medicine practitioner how light helps improve health, immunity and recovery, and he or she will likely compare it to acupuncture’s mechanism of action:
- Light is a form of energy, and our bodies are just big energy systems. Light has the power to stimulate specific meridian points and chakra zones in the human body.
- Red is said to stimulate the first chakra because it correlates most strongly with our survival instinct (hence why it gives us energy and makes us act quickly, in order to motivate us to pursue things like money, food, sex, power, etc.).
- While acupuncture uses tiny needles to achieve bodily harmony through stimulating certain points in the body’s energy system, light therapy uses focused, visible, red wavelengths in much the same way.
Red light has been shown to be naturally energizing and correlated with improved moods by increasing self-confidence, positivity, passion, joyfulness, laughter, social awareness, conversation skills and sensory stimulation. While results vary from patient to patient, there’s reason to believe that LLLT has mental and emotional perks in addition to physical benefits.
Red Light Therapy vs. Blue Light Therapy: What’s The Difference?
- Blue and red light therapies, two forms of phototherapy, have some similar benefits and uses, although they work in different ways. The mechanism of action of both is still not entirely well-understood, but it’s believed that LLLT devices produce light with wavelengths similar to those of blue light lasers only with broader output peaks (they’re less monochromatic and don’t produce heat or friction).
- Blue light is more commonly used at home from light-emitting devices, especially for the treatment of acne. It’s been found that blue light reaches the sebaceous (oil) glands in the skin and can help kill porphyrins, which are compounds inside acne bacteria. (12)
- Red light is believed to penetrate the skin deeper and may also help acne and other skin disorders by reducing inflammation and improving healing.
- Blue light and red light can be emitted from tabletop light therapy devices (which are used at home and usually weaker, requiring about a total of 30 minutes to one hour of treatment time twice per day) or from stronger devices used in doctors’ offices that work quicker (sometimes within just several minutes or less).
- The Wellman Center for Photomedicine at Massachusetts General Hospital explains that there’s still widespread uncertainty and confusion surrounding the mechanisms of action of these light therapies, especially LLLT, at the molecular, cellular and tissue levels. There are also a large number of parameters for doctors to consider before treating individual patients (wavelength, fluence, irradiance, treatment timing and repetition, pulsing, and polarization) that can add to the confusion and patient variability in terms of results. (13)
Where to Go and How to Use Red Light Therapy
Many conventional doctors consider red light therapies to still be alternative treatments, considering more research is needed overall to prove their efficacy and results can sometimes vary. Currently most medical insurance companies state that LLLT is an “experimental treatment” so many won’t provide insurance coverage. Depending on what condition you’re treating, you can speak with your dermatologist, oncologist, orthopedic, rheumatologist or neurologist about treatment options. Your primary care doctor, or a chiropractor, may be able to give you a referral.
Red Light Therapy Research and Historical Use
Different types of phototherapy light boxes have actually been used for decades to treat numerous mood-related, skin, sleep-related, and acute or chronic pain conditions.
A 2012 report published in Annals in Biomedical Engineering stated that red light is used in three primary ways: “to reduce inflammation, edema, and chronic joint disorders; to promote healing of wounds, deeper tissues, and nerves; and to treat neurological disorders and pain.” (14) It’s been found that red light therapy promotes stronger immunity and longevity by increasing cell proliferation and migration, as well as modulating levels of cytokines, growth factors and inflammatory mediators.
Starting in the late 1990s, NASA scientists began developing infrared light technologies that could be used for plant growth during shuttle missions. What they discovered over the past two-plus decades is that red light therapies could also provide healing cellular stimulation in humans and animals.
Here’s an overview of how red light therapy is believed to be effective:
Red light — even just seeing the color red — stimulates all of our senses, primes us for quick movement and deliberate action, and enhances courage. Because it grabs our attention, you’ve probably noticed that the color red is used on many warning signs and traffic signals in order to cut through clutter and alert us of danger. So what does the effect of seeing red have to do with healing?
Leanne Venier — an engineer, scientist and an expert in light frequencies and the healing effects of color therapy — explains that red light is naturally attention-getting, energizing, stimulating and “representative of survival, joy and passion” in humans because of how it affects of our central nervous system. According to her work, along with extensive research done by trustworthy organizations including NASA, red light can trigger the sympathetic nervous system and therefore activate the “fight or flight response.”
Being in fight-or-flight mode causes reactions like improved blood circulation, rapid heartbeats, increased sweating, high concentration and so on. Normally we think of activating our stress response as a bad thing, but this can also be healing because it carries nutrients to our cells and controls inflammatory responses.
Possible Side Effects/Cautions Regarding Light Therapy
Although red light therapy seems to be very well-tolerated and unlikely to cause side effects, it still remains controversial whether it can help all patients. One difficulty that researchers have had gathering results from studies on red light therapy is pinpointing which light ranges are optimal for treating different health conditions and different patients.
Certain published study results have found that LLLT can cause negative reactions when an inappropriate choice of light source or an inappropriate dosage is used. There is an optimal dose of light for any particular application, and in the case of red light therapy, often lower doses are found to be more effective than higher doses. Be sure to work with a qualified LLLT practitioner whenever receiving treatments, and report any side effects, including burning, swelling, dizziness, muscle weakness or nausea. Keep in mind that seeing results from red light treatments might take patience and that responsiveness is expected to vary.
Final Thoughts on Red Light Therapy
- Red light therapy (sometimes called LLLT or low level laser therapy) involves emitting red, low-light wavelengths through the skin to stimulate cellular rejuvenation, increase blood flow, stimulate collagen and more.
- Red light therapy/LLLT is used to help treat conditions such as cancer treatment side effects, wounds, wrinkles or fine lines, hair loss, arthritis symptoms, musculoskeletal disorders, and neurological damage.
- Red light therapy is well-tolerated by most, but results can vary. Researchers and experts feel there is still a lot to learn about how color/light laser therapies work, which means they remain controversial and not always covered by insurance.
New Study Shows That This Type Of Diet is Helpful for Hashimoto’s!
New Study Shows That This Type Of Diet is Helpful for Hashimoto’s!
By Dr. Izabella Wentz, Pharm D.
New Study Shows That This Type Of Diet is Helpful for Hashimoto’s!
Comments
Hot off the presses!
Can diet reduce your thyroid antibodies? A group of Italian researchers have recently published a study about the effects of nutrition on Hashimoto’s and they say “Yes”!
Over the course of 3 weeks, 180 people with Hashimoto’s were randomized to receive the study diet vs. a standard low calorie diet. 108 patients ate the study diet, while 72 patients served as the control group and followed a low calorie diet without any food restrictions or guidelines.
Thyroid antibodies (Thyroid Peroxidase antibodies (TPO antibodies), Thyroglobulin antibodies (TG antibodies) and antimicrosomal antibodies), TSH, free T3, free T4 as well as body weight, mass and composition was measured before the start of the study and after the study ended 3 weeks later in both the study group and the control group.
Here are the results of the study
Get this… after just 21 days, all the patients in the study group showed a significant decrease in the levels of thyroid antibodies, which are known to indicate how aggressive the attack is on the thyroid gland!! (The higher the antibodies, the more aggressive the attack, and I consider a drop of 10% or more an improvement!) This means that their condition was getting better!!
- Thyroglobulin (TG) antibodies dropped by 40% (−40%, P<−0.013)
- Thyroid Peroxidase (TPO) antibodies dropped by 44% (−44%, P< 0.029) Anti-microsomal antibodies dropped by 57%!! (−57%, P< 0.000)
In contrast, the people following the “normal diet” saw an increase in thyroid antibody markers!! This means that their condition was worsening...
- Thyroglobulin (TG) antibodies increased by 9% (+9%, P<0 .017="" span="">
- Thyroid Peroxidase (TPO) antibodies increased by 16% (+16%, P<0 .004="" 30="" anti-microsomal="" antibodies="" by="" increased="" nbsp="" p="" span="">
After 21 days, the study patients showed a slight decrease in body weight, body mass index and lost fat mass! “With regard to the body parameters measured in patients who followed this diet, reduction in body weight (-5%, P<0 .000="" and="" body="" index="" mass="" observed.="" p="" span="" were="">
Do you want to know more about the diet??
Here are the specifics of the study diet:
Low carbohydrate - The study diet program was based on the following guidelines: 12-15% carbohydrates, 50-60% proteins, and 25-30% fats (the standard Western diet contains 50% carbohydrates, 15% proteins, and 35% fats.
Veggie rich - Patients were told to eat vegetables, including large leafy greens (but to exclude goitrogens, see below).
Meats - Patients were told to eat only lean parts of red and white meat and were also allowed to eat fish
Excluded goitrogens - The authors quoted the following foods as goitrogenic: “cruciferous [vegetables] (Brassicaceae) family (rapeseed or canola, cabbage, turnip, watercress, arugula, radish, horseradish), milk, soy, spinach, millet, tapioca, and lettuce. Even certain food additives, ie, nitrates used for fish and meat preservation [were considered goitrogens].”
Also excluded: eggs, legumes, dairy products, bread, pasta, fruit and rice.
The Root Cause Approach
I was really excited to see that a diet very similar to what I’ve been recommending since 2012 now has research to back it up!!
If you’re new to my work, here are my dietary guidelines in a nutshell that align with the study:
I always recommend a diet that is gluten free (due to sensitivity in up to 88% of people with Hashimoto’s), free of soy, canola and rapeseed, due to potential goitrogenic properties that have been found to be an issue in Hashimoto’s.
I also recommend avoiding dairy products (not due to goitrogen content, but rather due to dairy protein sensitivity that is present in up to 80% of people with Hashimoto’s).
I do recommend eating nitrate free meats when possible and limiting processed foods and meats in general.
In many cases, I do recommend an autoimmune Paleo diet (excludes grains like rice and corn, excludes legumes and eggs in addition to nuts and seeds. I will often recommend staying off millet for advanced cases of Hashimoto’s, as it is a seed which can be reactive in some, with tapioca/cassava I recommend moderation due to starchy content. In some cases, I may also recommend a restriction of fruit.
Here are the differences between the study and my recommendations:
I previously wrote a post about goitrogens—a goitrogen is any substance that interferes with thyroid function—the tricky part is that not all of them are created equally and not all of them work in the same way.
Overall, my position on goitrogens in the crucifer family like broccoli, cabbage, turnip and the like has been that they are healthy for most people with Hashimoto’s and that they help the body detoxify, especially when cooked, fermented or lightly steamed, but even in their raw state. I have not seen issues with cruciferous vegetables in most clients, with the exception of those with small intestinal bacterial overgrowth (SIBO) (because crucifers are high in FODMAPs, which aggravate SIBO), and in those with the CBS genetic mutation (due to high sulfur content of crucifers).
Lettuce is hardly ever something I recommend avoiding, with the exception of some cases of irritable bowel syndrome, as any raw veggies can aggravate IBS and we know that lettuce is not exactly a cookable thing ;-)
Fat vs. protein vs. carb ratios - I often have people play around with their fat to protein to carb ratios to eat what fits them best. Some people (especially if they’re more active) will benefit from more proteins. Others benefit from more fats, such as those with brain fog, pain and depression. Some may even benefit from ketosis. Personally for me, lower carbs, higher fats and ketosis made me feel amazing for a couple of years, until I hit a plateau and then needed to add back more carbs to feel my best. The bottom line is that you have to adjust the diet to your needs and your needs may change!
Critique of the study
It’s difficult to tell whether the carb restriction, goitrogen restriction, avoiding highly reactive foods (gluten, dairy, soy, eggs), or all of the above, played a role in improving patient outcomes.
I personally have seen similar results with thyroid antibodies reducing—and sometimes going away—and symptoms like fatigue, brain fog, anxiety, IBS and pain virtually disappearing and weight and hair loss beginning to decline in as little as three weeks with carb restriction and avoiding reactive foods! I am not sure what role goitrogens play at this point… If you are already eating low carb and avoid reactive foods and are interested in being a “guinea pig” for three weeks and also remove goitrogens, I’d love for you to report back to me on what results you found!
I would love to see a study that isolated goitrogens vs. low carb diet vs. allergen avoidance. Until then, I’m happy with interest in this direction and will look forward to hearing from my fellow root cause rebels who decide to take on the guinea pig challenge.
I wish that the control group was an actual control group (the control group should have kept eating their “normal” diet), and I also wish that low-calorie was defined. How low are we talking? 800 Calories? 1200 Calories? 1500 Calories?? Obviously there’s a big difference between 800 and 1500 Calories!
There was very little talk about adherence. Were the study participants actually following the diet they were told to follow? Was the control group actually eating low calorie? (adherence is a challenge for many studies of this sort).
Another critique of this study is that I wish the study had been done for at least 3 months, as that is the time needed to see the full effect on thyroid antibody markers!
**In reading the introduction and conclusion, it seems that the patients following the low-carb, low-goitrogenic diet saw a reduction in thyroid antibodies and weight markers. However, in reading the results, it looks as though the low-calorie group lost the weight? In my experience, losing weight in either scenario is going to happen, at least within three weeks (those in the low calorie group are more likely to gain it back, while the ones in low-carb group won’t gain the weight back but may eventually plateau if their adrenals are still out of balance -> 90% of people with Hashimoto’s have some degree of adrenal dysfunction in my practice -> Here’s a post about adrenals). I’ve reached out to the researchers for clarification.
Additionally, it would have been great to track patient symptoms in addition to weight because, after all, we all want to not just look better but also feel better!!
Busting Common Hashimoto’s Diet Myths…
I’m really excited that this diet is busting common Hashimoto’s diet myths.
Some people think that going gluten free is only beneficial in people who have both Hashimoto’s and Celiac disease, but none of the patients in this study were found to have Celiac disease! All of them did have Hashimoto’s, and all of the patients who followed the study diet had a reduction in thyroid antibodies!
Many people with Hashimoto’s are also dairy sensitivity (up to 80% felt better in my survey). Interestingly, the study reported that 83% of people with thyroid antibodies had a deficiency in lactase, which is an enzyme that digests lactose in milk. In my experience, the casein in milk is more of a problem than the lactose, however.
Have you heard the myth that a low carbohydrate diet is “bad” for Hashimoto’s? Again, this is a common myth, but this study has shown that this is not the case and that low-carb is actually beneficial. Furthermore, I’m excited to see evidence that supports eating proteins and fats :-)
So what about the goitrogen myth? I still hold my original stance but am willing to re-evaluate this position given more evidence. If you are already eating low carb and avoid reactive foods and are interested in being a “guinea pig” for three weeks and also remove goitrogens, I’d love for you to report back to me on what results you found… because after all, how you feel is most important!!
Conclusion:
If you would like to reduce your TPO antibodies, reduce your TG antibodies and feel better (and potentially lose up to 5% of your weight), try the following plan for three weeks!
- Free of highly reactive foods (gluten, grains, eggs, soy, dairy, legumes)
- Low carbohydrate diet (low in fruit too!)
- Rich in veggies (maybe even limit goitrogens?)
I hope this helps you on your journey!!
Why Hydrogen Peroxide Should be in every home
Why hydrogen peroxide should be in every home
Sunday, October 30, 2016 by: David Gutierrez, staff writer
Tags: hydrogen peroxide, natural cure, cosmetics
Tags: hydrogen peroxide, natural cure, cosmetics
========================
(NaturalNews) Inexpensive, nontoxic, versatile and potent: Hydrogen peroxide is a wonder product that belongs in every home.
Hydrogen peroxide is widely known as a disinfectant for minor cuts and scrapes, but many people don't understand that it works simply by oxidizing microbes to death. Hydrogen peroxide is simply water with an extra oxygen atom attached; in this unstable form, the oxygen breaks off from the water and forms a free radical solution that is highly reactive. But once it has reacted, the only byproducts are non-reactive oxygen and water. This is why, when used properly, hydrogen peroxide is so safe.
Hydrogen peroxide is so safe and effective that our own immune systems actually generate it as the first line of defense against microbes as diverse as bacteria, viruses, yeast and parasites. In this context, it also appears to act as an anti-inflammatory.
Natural remedies
So how can you make hydrogen peroxide work for you? Unsurprisingly, many of this product's greatest uses are as natural cures or for some other health-promoting function. For example, a nasal spray made from one tablespoon of 3 percent hydrogen peroxide in a cup of non-chlorinated water can be an effective treatment for sinus infections. Toothaches caused by minor infection can be treated with a hydrogen peroxide mouthwash; the same mouthwash can also remove bad breath.
If you think you're coming down with a cold, stave it off by placing a few drops of hydrogen peroxide in your ears each morning.
Hydrogen peroxide is also a potent anti-fungal. A 50–50 mix of hydrogen peroxide and water, sprayed on the feet every night and allowed to dry, is a good way to get rid of athlete's foot and other fungal infections. A similar (but much more diluted) cure can be used on plants suffering from fungus; in this case, dissolve half a cup of hydrogen peroxide in a gallon of water and spray on the affected plant.
Replace your cosmetics!
You can also get lots of use from hydrogen peroxide around the home. Mixed with baking soda, it makes a great toothpaste. It can also be used to protect water that you expect to be standing for a while, such as that in a humidifier or steamer – a pint of hydrogen peroxide mixed in will prevent microbial growth. Similarly, you can use hydrogen peroxide as a toilet bowl cleaner; let it sit for 20 minutes and then scrub.
When properly diluted, hydrogen peroxide can detox your skin by stripping away harmful environmental toxins. Just mix 2 quarts of hydrogen peroxide into a full bathtub and soak for half an hour or more.
Other cosmetic uses of hydrogen peroxide include cleaning your contact lenses – it denatures proteins that build up on the lenses – or helping to remove ear wax buildup. A few drops in the ears, followed by a few drops of olive oil, will cause earwax to break up and drain out.
Hydrogen peroxide can also be used as a safer, gentler alternative to bleach for lightening your hair.
Household uses
Hydrogen peroxide isn't just for your body; it can also be for your dog's! Hydrogen peroxide can induce rapid vomiting in dogs that have swallowed dangerous objects. Vomiting should only be induced upon a vet's recommendation, however.
Finally, hydrogen peroxide can be great for your clothing. Use it instead of bleach to whiten your laundry. More carefully applied, it can take out organic stains by breaking apart the proteins causing the discoloration. This is particularly effective with blood.
Use caution when applying hydrogen peroxide directly to clothing, as it may bleach or discolor some fabrics. But if you have a fresh, organic stain, you should be fine if you pour on just a small amount of hydrogen peroxide, wait a few minutes (it should foam), and then rinse it off with cold water and soap.
Sources for this article include:
Saturday, October 29, 2016
What is not healthy in your home Joe Mercola MD
10 Things You Think Are Healthy, but Aren't
September 16, 2015 | 711,733 views
By Dr. Mercola
Awareness is increasing that many household goods, from your personal care products and food packaging to your couch cushions, could harbor dangerous chemicals. Less well known is the fact that even seemingly healthy products may turn out to be bad for you.
If you have any of these "healthy" or at the very least innocuous-seeming items around your home, you may want to think twice…
10 'Healthy' Items Your Home Is Better Off Without
1. Antibacterial Soap
Washing your hands is your number one protection against the acquisition and spread of infectious disease. But you do not need to use antibacterial soap to get the job done.
Studies have shown that people who use antibacterial soaps and cleansers develop a cough, runny nose, sore throat, fever, vomiting, diarrhea, and other symptoms just as often as people who use regular soaps.1
Part of the reason for this is because most of these symptoms are actually caused by viruses, which antibacterial soaps can't kill. But even for symptoms like vomiting and diarrhea, which may be caused by bacteria, using antibacterial soaps will offer you no advantage over plain soap and water.2
So, the rational conclusion is antibacterial soaps are completely unnecessary for the purpose of washing away bacteria.
A 2007 systematic review published in the journal Clinical Infectious Diseases confirmed that antibacterial soap containing triclosan did not provide any additional benefit compared with a non-antibacterial soap.3
Antibacterial soap, will, however, expose you to triclosan, an antibacterial chemical that has been linked to concerns over antibiotic resistance and endocrine disruption.
Some animal studies showed that triclosan caused fetal bone malformations in mice and rats, which may hint at hormonal effects. Triclosan has also been found to cause estrogenic activities in human breast cancer cells, which may stimulate the growth and development of cancer cells.4
2. Your Chair
An error occurred.
At the molecular level, your body was designed to be active and on the move all day long. When you stop moving for extended periods of time, such as by sitting, it's like telling your body it's time to shut down and prepare for death.
Research published in the Journal of the American College of Cardiology, for instance, showed that women who sit for 10 or more hours a day may have a significantly greater risk of developing heart disease than those who sit for five hours or less.5
Research published in Diabetologia also found that those who sat for the longest periods of time were twice as likely to have diabetes or heart disease, compared to those who sat the least.6 Sitting for more than eight hours a day has also been associated with a 90 percent increased risk of type 2 diabetes.7
Excess sitting may increase your risk of colon, breast, and endometrial cancers, and the more hours you spend sitting in a day, the shorter your lifespan may be.
One study found, for instance, that reducing the average time you spend sitting down to less than three hours a day could increase your life expectancy by two years.8
The evidence is overwhelming at this point — 10,000 studies and growing — that prolonged sitting will reduce your lifespan by promoting dozens of chronic diseases, even if you exercise regularly. I believe the answer is to stand up as much as possible (aiming for less than three hours of sitting daily).
If you work a desk job, a standing workstation will be instrumental for achieving this goal, and I also recommend getting 10,000 steps a day via daily walk, in addition to regular high-intensity exercises.
3. Whitening or Antibacterial Toothpaste
Whitening toothpastes may be grittier in order to scrub stains off your teeth, but the grit may actually wear away your enamel or make your teeth and gums more sensitive. Also be on the lookout for antibacterial toothpaste, like Colgate Total, which contains triclosan.
In addition, many commercial brands may be loaded with toxic toothpaste ingredients, like sodium lauryl sulfate (SLS), artificial sweeteners, fluoride, propylene glycol, and microbeads. The latter pose a risk to the environment and have been found getting trapped under patients' gums.
This gives food and bacteria an entrance to your gum line, which could actually cause gum disease.9 It's possible to make your own toothpaste and avoid many of the pitfalls of commercial varieties. You can find two homemade toothpaste recipes here.
4. Cotton Swabs
Your ears should have a healthy amount of earwax, as they're a self-cleaning part of your body. Excess earwax should move out of your ear canal automatically, as cells there actually migrate naturally.
The removal of earwax is also helped along by movements of your jaw (talking, chewing, etc.), and once it reaches your outer ear it will simply fall out or be removed when you shower or bathe.
According to the American Academy of Otolaryngology – Head and Neck Surgery Foundation (AAO-HNSF), under ideal circumstances your ear canals should never have to be cleaned, especially with cotton swabs. They state:10
"Unfortunately, many people mistakenly believe that earwax should be routinely removed for personal hygiene. This is not so. In fact, attempting to remove earwax with cotton-tipped swabs, bobby pins, or other probing devices can result in damage to the ear, including trauma, impaction of the earwax, or even temporary deafness.
These objects only push the wax in deeper, and can block the ear canal entirely."
Under normal circumstances, earwax is only produced in the outer one-third of your ear canal. One of the primary risks of cotton swabs is they can push the earwax into the deeper part of your ear canal, near the eardrum. As AAO-HNSF noted:11
"When a patient has wax blockage against the eardrum, it is often because he has been probing the ear with such things as cotton-tipped applicators, bobby pins, or twisted napkin corners. These objects only push the wax in deeper."
When earwax is pushed deep into your ear where it doesn't belong, it can bring fungus, bacteria, and viruses from the outer ear into the inner ear, increasing the risk of infection. It can also block your ear canal, leading to hearing loss, or even cause a ruptured eardrum.
It's a vicious cycle, too, because the more you rub your ears with cotton swabs, the more histamine will be released, which makes your skin irritated and inflamed. This, in turn, may make you want to insert a cotton swab again, leading to additional dryness and irritation.12
5. Humidifier
During the winter months, heaters and cold temperatures may lead to dry air with low humidity. This dry air can lead to dry skin, irritated sinuses and throat, and itchy eyes. Over time, exposure to low humidity can even dry out and inflame the mucous membrane lining your respiratory tract. When this natural barrier is no longer working properly, it increases your risk of colds, the flu, and other infections.
You may be tempted to add humidity to your home's air using a humidifier, and this is a sensible solution as long as it doesn't backfire. You must be very careful about making sure your humidity levels are not too high, as high humidity will cause mold to grow, which could devastate your health.
Additionally, the moist, warm environment of a humidifier is a breeding ground for bacteria and fungi, which travel out of the unit via a "toxic mist" that you later breathe in.
Research has shown that breathing in dirty mist from humidifiers can lead to lung problems, including infection, and humidifier use is actually associated with an increased risk of developing asthma in children.13 So if you choose to use a humidifier, do so sparingly, making sure humidity levels do not get too high. A hygrometer, which you can find at most hardware stores, can measure the amount of moisture in your home's air so you can adjust your humidifier use accordingly. Some humidifiers also have a hygrometer built in.
According to Dr. Robert Ivker, D.O., former president of the American Holistic Medical Association, the ideal level of relative humidity for sinus health is between 35 to 45 percent. This level is also generally recommended to avoid mold damage in your home. As far as using a humidifier goes, you'll also need to make sure you clean it often, at least once every three days using hydrogen peroxide to remove any film or mineral deposits.
The water in the reservoir should be changed daily, and be sure the area around it (tabletops, windows, carpeting, curtains, etc.) are kept dry. If you have a central air heating system, the best humidifier is one that is built directly over your furnace and tied into a humidistat and water source so the entire process is automated and your home is evenly humidified.
6. Loofah
A loofah provides a perfect environment for bacteria, fungi, and mold to grow, especially when kept in the warm, humid confines of your bathroom or shower. As you run it over your skin, it's possible that small wounds (including tiny nicks from shaving) could be infected, leading to impetigo, folliculitis, or other skin issues.14 If you love to loofah, choose one made of a natural fiber, which will naturally contain enzymes to inhibit microbial growth, and replace it monthly. After each use, wring it out and allow it to dry thoroughly – and store it in a cool, dry spot.
7. Blender
Blenders are handy for whipping up healthy morning smoothies… but if you're not washing yours properly, it could be a problem. The blender gasket (the rubber ring that holds the blade portion of the blender in place) has been found to be the third germiest item in the kitchen, and research showed it commonly harbored salmonella, E. coli, yeast, and mold.15 The solution is simple – when you're done using your blender, be sure to disassemble it completely and wash each part, including the gasket, well.
8. Nail Tools
Pumice stones, cuticle clippers, and other nail tools harbor bacteria from your skin. If you neglect to wash them, they could potentially cause skin infections (this is especially true if you share your nail tools with friends or family members). Nail tools should be washed with soap and water after each use, and pumice stones should be replaced every three to four weeks.
9. Rubber Spatula
Rubber spatulas were found to be even germier than blender gaskets, coming in at the second germiest item in the kitchen. The problem is that most people do not pull the spatula head off the handle when cleaning, which allows E. coli, yeast, and mold to grow. If your spatula comes apart, always remove the head and wash each piece separately. If not, pay special attention to the joint between the head and the handle when washing.
10. Stuffed Animals
Stuffed animals are known to collect dust mites, which are a major cause of indoor dust allergies. If you're allergic, exposure can lead to sneezing, runny nose, itchy eyes, and other symptoms. If your child can't part with theirs, cut the number down to one or two kept on the bed, with the rest stored on a shelf. You can also put the stuffed animals in a plastic bag and leave it in the freezer overnight, as the cold will kill the dust mites.
Do Scented Candles, Incense, and Air Fresheners Cause Cancer, Allergies, and Asthma?
Many people enjoy the ambience that scented candles, incense, and air fresheners can add to their home, but with that pleasant scent come some hidden health risks. Such products are known to contain volatile organic compounds (VOCs), allergens, phthalates, and cancer-causing chemicals such as benzene and formaldehyde. Many of the chemicals emitted by these products have been linked to hormone disruption, allergies, asthma, and even cancerous mutations in DNA.
In one recent study, scented candles were found to act as potent sources of VOC emissions whether they were lit or not, and when lit, formaldehyde had the highest emission concentration.16 Incense sticks and air fresheners have also been shown to contribute to poor indoor air quality, including the release of benzene.17 The Daily Mail further reported:18
"In 2013, after a study of more than 2,000 pregnant women, the International Journal of Public Health reported that women who used air fresheners in their homes were significantly more likely to have babies that suffered from wheezing and lung infections. One study that followed 14,000 children from before and after birth found they had higher levels of diarrhea and earache, while their mothers had raised risks of headaches and depression, all linked to the frequent use of air fresheners and aerosols during pregnancy and early childhood.
A 2007 study also found that using air fresheners as little as once a week can raise the risk of asthma in adults. The same report found that the risk of developing asthma was up to 50 percent higher in people who had been exposed to air-freshener sprays."
Chemicals in Personal Care Products Linked to Increased Risk of Miscarriage
Chemicals known as phthalates, which are used as plasticizers in everything from vinyl flooring to detergents, hoses, raincoats, adhesives, air fresheners, and toys — and even in many soaps, shampoos, lotions, nail polish, and other personal care products.
Phthalates are one of the groups of "gender-bending" chemicals causing males of all species to become more female. Research conducted by the U.S. Centers for Disease Control and Prevention (CDC) discovered high levels of phthalates in all 289 adult Americans tested, and the levels of some phthalates in women of childbearing age exceeded the government's safe levels set to protect against birth defects, leading scientists to conclude phthalate exposures are "much higher and more common than previously suspected.19
A new study also revealed that women with higher levels of phthalates in their urine were more likely to have miscarriages between 5 and 13 weeks of pregnancy than those with lower levels.20 These chemicals have disrupted the endocrine systems of wildlife as well, causing testicular cancer, genital deformations, low sperm counts, and infertility in a number of species, including polar bears, deer, whales, and otters, just to name a few. Scientists believe phthalates are responsible for a similar pattern in humans as well, and they have been linked to:
|
Impaired ovulatory cycles and polycystic ovary disease (PCOS)
|
"Decreased dysgenesis syndrome": A syndrome involving cryptorchidism (undescended testicles), hypospadias (birth defect in which opening of urethra is on the underside of the penis instead of at the end), oligospermia (low sperm count), and testicular cancer
|
|
Interference with sexual differentiation in utero
|
Enlarged prostate glands
|
|
Disturbed lactation
|
Numerous hormonal disruptions
|
|
Early or delayed puberty
|
Breast cancer and uterine fibroids
|
How to Create a Healthier Home
While it's important to carefully wash items like your blender to remove germs, and replace loofahs regularly to avoid infections, by far the greatest risks in your home come from the chemicals in common household products. The fewer ingredients a product contains, the better, and try to make sure anything you put on or in your body – or use around your home – contains only substances you're familiar with. If you can't pronounce it, you probably don't want it anywhere near your family. The following tips will help you to create a healthier home, naturally.
- As much as possible, buy and eat organic produce and free-range, organic meats to reduce your exposure to added hormones, pesticides, and fertilizers. Also avoid milk and other dairy products that contain the genetically engineered recombinant bovine growth hormone (rBGH or rBST).
- Rather than eating conventional or farm-raised fish, which are often heavily contaminated with PCBs and mercury, supplement with a high-quality purified krill oil, eat smaller fish, or fish that is wild-caught and lab tested for purity. Wild caught Alaskan salmon is about the only fish I eat for these reasons.
- Buy products that come in glass bottles or jars rather than plastic or canned, since chemicals can leach out of plastics and into the contents.
- Store your food and beverages in glass rather than plastic, and avoid using plastic wrap.
- Use glass baby bottles and avoid plastic sippy cups for your little ones.
- Eat mostly raw, fresh foods. Processed, prepackaged foods (of all kinds) are a common source of chemicals such as BPA and phthalates.
- Replace your non-stick pots and pans with ceramic or glass cookware.
- Filter your tap water — both for drinking and bathing. If you can only afford to do one, filtering your bathing water may be more important, as your skin absorbs contaminants. To remove the endocrine-disrupting herbicide Atrazine, make sure the filter is certified to remove it. According to the Environmental Working Group (EWG), perchlorate can be filtered out using a reverse osmosis filter.
- Look for products that are made by companies that are earth-friendly, animal-friendly, green, non-toxic, and/or 100% organic. This applies to everything from food and personal care products to building materials, carpeting, paint, baby items, upholstery, and more.
- Use a vacuum cleaner with a HEPA filter to remove house dust, which is often contaminated with traces of chemicals.
- When buying new products such as furniture, mattresses, or carpet padding, ask what type of fire retardant it contains. Be mindful of and/or avoid items containing PBDEs, antimony, formaldehyde, boric acid, and other brominated chemicals. As you replace these toxic items around your home, select those that contain naturally less flammable materials, such as leather, wool and cotton.
- Avoid stain- and water-resistant clothing, furniture, and carpets to avoid perfluorinated chemicals (PFCs).
- Minimize your use of plastic baby and child toys, opting for those made of natural wood or fabric instead.
- Only use natural cleaning products in your home or make your own. Avoid products that contain 2-butoxyethanol (EGBE) and methoxydiglycol (DEGME) — two toxic glycol ethers that can damage fertility and cause fetal harm.21
- Switch over to organic brands of toiletries such as shampoo, toothpaste, antiperspirants, and cosmetics. You can replace many different products with coconut oil and baking soda, for example. EWG has a great database22 to help you find personal care products that are free of phthalates and other potentially dangerous chemicals. I also offer one of the highest quality organic skin care lines, shampoo and conditioner, and body butter that are completely natural and safe.
- Replace feminine hygiene products like tampons and sanitary pads with safer alternatives.
- Avoid artificial air fresheners, dryer sheets, fabric softeners, or other synthetic fragrances.
- Look for products that are fragrance-free. One artificial fragrance can contain hundreds – even thousands – of potentially toxic chemicals.
- Replace your vinyl shower curtain with one made of fabric.
Why You Need to Use the Armpit Detox Recipe (or not use deodorants with these ingredients)
Why You Need to Use This Armpit Detox Recipe
Disease & Conditions, Healthy Living, Natural Solutions, Phthalates, self improvement, Tips, Toxin Exposure0
Pinterest
Many of the common household products we use every day are full of harmful chemicals and toxic ingredients, which seriously endanger our health.
One of the most threatening items is the deodorant. Despite containing many dangerous chemicals, like aluminum, these products are applied on a sensitive area, where there are major lymph nodes, and can be directly absorbed in the system, influencing the lymphatic system, the sebaceous glands, and the immune system.
If you read the ingredients of your deodorant you will be quite surprised. Namely, these are the most common ingredients of commercial deodorants:
Aluminum- Yes, you read it right. Our deodorants contain metals, which can cause severe adverse effects on our health. Studies have shown that aluminum is related to the onset of cancer and Alzheimer’s.
Formaldehyde— This chemical is used to preserve deceased bodies after death, it destroys germs and is a popular carcinogen.
Parabens– Parabens lead to a hormonal imbalance and have been discovered in the biopsies of breast cancer tissue.
Phthalates— Phthalates are also included in plastic and affect the hormones as endocrine disruptors. They have also been related to infertility in men.
Propylene glycol- This is, in fact, antifreeze, the chemicals used to cool the car, which can kill your pets; applied on the underarms via deodorant. According to the Environmental Working Group reports, its use in our common personal care products increases the risk for allergies and immunotoxicity.
Antibacterial Substances- These ingredients can weaken the immunity and pose a risk when it comes to superbugs.
When you consider all the potential hazards of the use of deodorants, you are already aware of the need to another alternative to these products.
You may want to try some chemical- free deodorant or a magnesium spray which will eliminate the bad odor, but an armpit detox is definitely what will solve your problem the best. It will remove the dangerous chemicals from the sweat glands, the underlying tissue, and the skin while providing a great smell.
Sometimes, the switch to natural deodorants may cause rashes, so the armpit detox will soothe them and also reduce the sweat.
You can feel the difference by doing a simple armpit detox which requires only 30 minutes of your time. Yet, we recommend that you repeat it on a few days until your body gets used to the natural deodorants.
Armpit Detox Recipe
Apple cider vinegar is a potent cleansing agent which removes the toxins as soon as it comes into contact with the skin. Yet, make sure you always use organic one with the “mother” on the bottom.
As soon as it is mixed with water, Bentonite clay can provide magnified effects. It will dry like a clay mask while cleansing the skin on the surface. It will cleanse the pores deeply and destroy bacteria.
Ingredients:
- 1 teaspoon Apple Cider Vinegar
- 1 tablespoon Bentonite clay
- 1-2 teaspoons of water (until you get the right consistency)
Instructions:
In a suitable bowl not made of metal, mix the ingredient with a wooden spoon and stir until you get a creamy mixture.
Then, spread the mixture on the armpits with the fingers or a cloth. Leave it to act for 5-20 minutes.
You should leave it less the first time, and gradually increase the time afterward. After some time, wash it off with warm water in the shower or using a washcloth.
You may experience a slight warming sensation or tingling in the beginning until the body gets used to the substances. Yet, if it hurts, wash it out with water and try some other detox recipe. The redness is normal, it indicates that the blood flow in the area has been improved.
Repeat every few days or until you notice that the natural deodorant does not irritate the skin anymore.
Additional notes:
- Many people claim that after this detox procedure, they no longer need baking soda in the natural deodorants they use.
- Make sure you drink plenty of water in order to hydrate the body and help it flush the toxins.
- If you still have lumps in the armpit, try gentle dry brushing (gently) or a massage of the area once a day.
Source(s):
healthyfoodstar.com
losingweightdone.com
Thursday, October 27, 2016
Tuesday, October 25, 2016
Monday, October 24, 2016
Reducing Cancer Risk Pueraria mirifica
Pueraria mirifica and Reducing Cancer Risk
An Interview with Phytoestrogen Expert, Professor Margaret Ritchie
By Richard A. Passwater, Ph.D. - October 24, 2016
16
{kind=link}
/11013167/InPost_LB
/11013167/InPost_LB_Mob
Last month, we discussed the effectiveness of the herb Pueraria mirifica against menopausal symptoms with Christiane Northrup, M.D. (1). It had been almost 10 years since we discussed the effectiveness and safety of P. mirifica and I wanted to update readers on both the effectiveness and the protection against breast cancer (2, 3). In the 2007 interviews with Dr. Garry Gordon, he presented epidemiological evidence that P. mirifica lowered the risk of breast cancer. To me, that almost seemed to verge on being too good to be true. At a time when the popular pharmaceutical was being associated with increased risk of breast cancer, how could a natural herb be more effective and, at the same time, lower the risk of cancer? This would be extremely important to all women. I needed laboratory and clinical evidence as well as the epidemiological evidence presented by Dr. Gordon.
My first step was to seek out the world’s best authority in phytoestrogens and cancer. My research indicated that this is Professor Margaret Ritchie, Ph.D., of Dundee University and the University of the West of Scotland. My second step was to visit her laboratory and observe her team of researchers studying P. mirifica’s actions against cancer cells. Professor Ritchie’s publication of a validated database of phytoestrogens blazed the way for many other phytoestrogen researchers to follow.
Dr. Ritchie has a background in pure chemistry from the University of St. Andrews and a passion for the role of phytochemicals on health. Her academic studies include further qualifications and research in the therapeutic use of plant-based bioactive compounds. She was a research Theme Leader in PhytoChemicals at the Bute Medical School, University St. Andrews and has experience in identifying biomarkers of phytochemical intake and performing clinical studies testing the pharmacological activity of herbal medicinal drugs and nutraceuticals.
She was the first researcher in the world to identify biomarkers of phytoestrogen intake and create a validated database of phytoestrogen content of foods. Dr. Ritchie led research at St. Andrews, Dundee and Edinburgh Napier Universities and collaborated in several of the largest European studies investigating the impact of phytochemicals and nutrition on cancer.
She was the Royal Society of Chemistry Education Coordinator for Scotland and advisor to the Higher Education Training Council for Ireland.
Dr. Ritchie has recently taken up new posts with the University of Dundee and the University of the West of Scotland. She is also an accreditation assessor for the Association for Nutrition and a visiting lecturer.
She is currently a member of the National Advisers and Inspectors in Science and a member of the editorial board for the Journal of Nutrition and Food Science.
Passwater: Professor Ritchie, what led to your interest in phytoestrogens?
Ritchie: My major interest has always been in chemistry and while completing my first degree in pure chemistry at the University of St. Andrews, a close relative suffered from cancer. As a result of this personal experience, I decided to use my knowledge of chemistry to try and help in the management of disease, in particular, cancer. By management, I would suggest the prevention as well as the treatment of disease.
I completed further studies after graduating from St. Andrews University and during that time I became fascinated with the actions, properties and potential role of plant chemicals on human health. I learned that plants contain a huge variety of bioactive compounds (i.e., compounds that can promote an effect on the body or tissue or cell). At this point, I decided to find out more about the role of plant chemicals and investigate their properties through research.
After attending a lecture about breast cancer by a surgeon and during subsequent conversations with him and with breast cancer patients, I became aware of increased media attention about breast cancer and research that was being undertaken on phytoestrogens. After following up research leads in the field of breast and prostate cancer, I met staff at Tenovus in Cardiff, Wales, who inspired me to carry out research into phytoestrogens. A key person who trained me in phytoestrogen analysis was Dr. Mike Morton. Dr. Morton and Professor Griffiths (another expert in phytoestrogen research and hormone dependent cancers) were both based at Tenovus, Cardiff.
Passwater: Phytoestrogens seem to be confusing to many health professionals, especially those who do not specialize in them. How long have you been researching them?
Ritchie: I have been researching the properties of phytoestrogens for over 15 years. Although they form the main group in which I have a significant interest and they have been the basis of the majority of my research, I have carried out research involving human trials and other bioactive plant compounds. During my research involving phytoestrogens, I created a validated database containing information about the amount of the common phytoestrogens in food and subsequently, I identified biomarkers of intake using blood and urine samples. I then investigated the effect of intake and exposure of phytoestrogens on the risk of breast cancer and on patients who had been diagnosed with breast cancer.
Passwater: What led your interests to P. mirifica?
Ritchie: During my visit to Tenovus in Cardiff and my meeting with experts in the field of cancer and phytoestrogens, there was a reference to miroestrol, which along with its “sister” compound, deoxymiroestrol, are the most active phytoestrogens in P. mirifica. I was very keen to investigate this herb further. I was also completing several research studies at St. Andrews University and the preliminary results indicated that exposure to phytoestrogens may be beneficial to both breast and prostate cancer patients prior to diagnosis.
Passwater: Okay, let’s start with the basics. What are phytoestrogens?
Ritchie: Phytoestrogens are a group of compounds produced naturally by edible plants. The word “phyto” comes from the Greek word for plants. The term “phytoestrogen” refers to the ability of such compounds to mimic the biological effects of estrogens by binding to and subsequently, activating, the nuclear estrogen receptors.
Passwater: What are estrogens and how do they work?
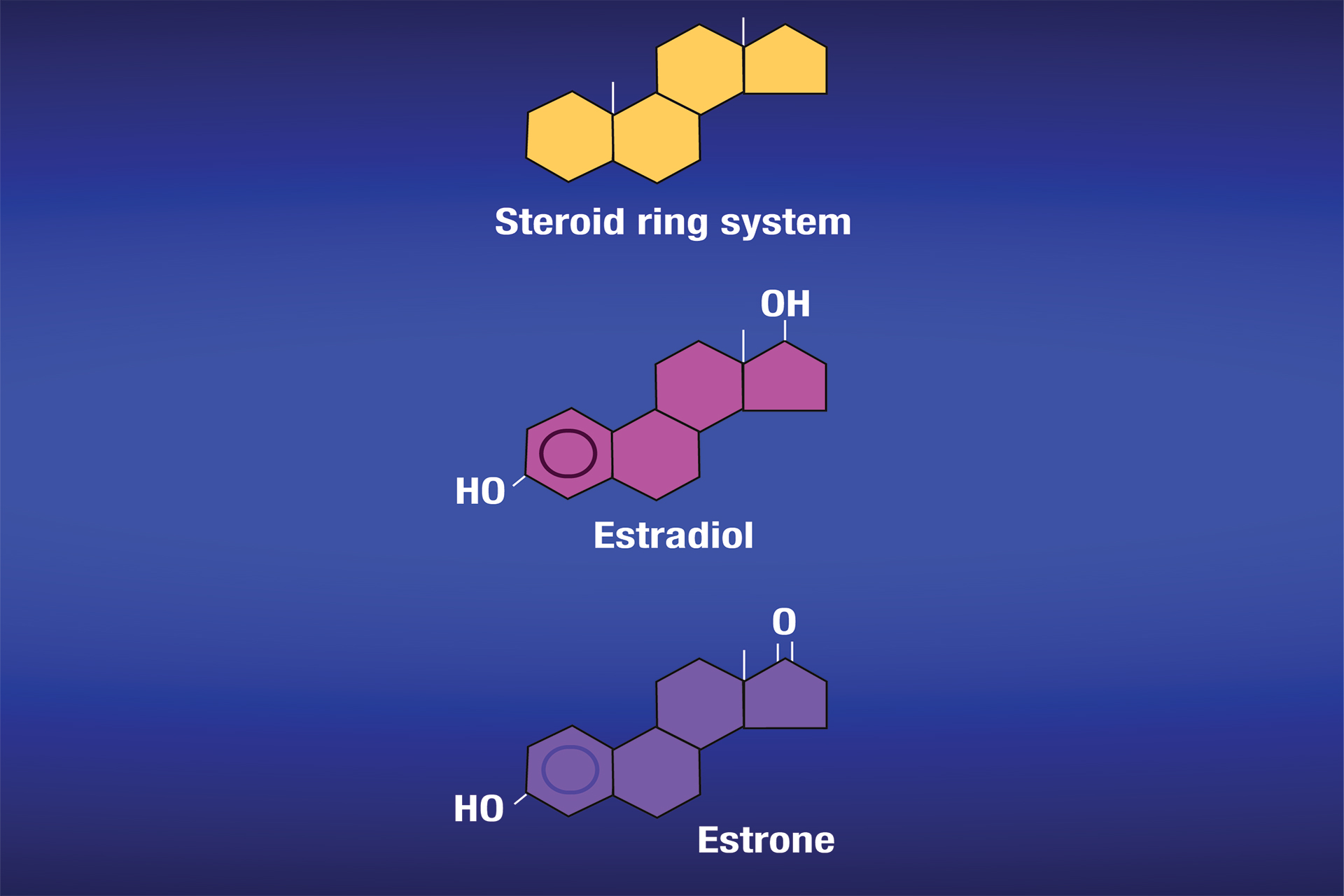
Ritchie: “Estrogens” refers to a group of hormones with similar chemical structures (see Figure 1) produced in the body from a variety of tissues. Hormones are produced in glands and then travel in the blood to their target tissues. Estrogens are present in both men and women, and they have functions in both, although their levels in women tend to be higher. They have a variety of functions, especially in women during sexual and reproductive development. They can also be known as female sex hormones.
{kind=link}
Figure 1: Estrogens belong to the steroid family of compounds. The top schematic shows the general four-ring system of steroids. The rings are identified as (left to right) A, B, C and D rings. Estradiol and estrone are two common estrogens of interest. As shown in the middle schematic, the estrogen estradiol has two hydroxyl groups (OH), one is attached to the “D” ring (the outermost ring on the right) and the other to the “A” ring (innermost ring on the left). The bottom schematic shows the estrogen, estrone, which has only one hydroxyl group, which is located on the “A” ring and it has a ketone radical (=O) on the “D” ring. A third important estrogen is estriol (not depicted), which has three hydroxyl groups. Two hydroxyl groups are attached to the “D” ring and one to the “A” ring. Courtesy of National Cancer Institute.
Estrone, estradiol and estriol are the three of the most common estrogens. A fourth estrogen, estetrol, is produced only during pregnancy. It is worth noting that estradiol tends to be present in greater quantities in women of reproductive age. Estriol is the main estrogen produced during pregnancy. Estrone is normally the only estrogen produced after menopause. In other words, estradiol is the more prominent estrogen in non-pregnant females between puberty and menopause; during pregnancy estriol becomes the more prominent; and after menopause, estrone becomes the primary estrogen.
Estrogens are produced from cholesterol. Initially, cholesterol is converted to pregnenolone, which is subsequently converted to progesterone. Progesterone then undergoes conversion into several male hormones including testosterone. Estradiol and estrone can be produced from testosterone. Estriol tends to be produced in large quantities during pregnancy, as I mentioned.
Estrogens are responsible for physical changes during puberty in females, which include the start of menstruation and the development of breasts and underarm hair. Estrogens are also responsible for protecting bone health (in both men and women), maintaining cholesterol levels and they can affect mood. The can also affect the lungs and heart.
The ovaries, which produce a woman’s eggs, are the main source of estrogens in women. Also, the adrenal glands, located at the top of each kidney, make small amounts of estrogens in both women and men. So does fat tissue. Estrogens circulate in the blood and act nearly everywhere in the body (see Figure 2).
{kind=link}
Figure 2: The primary target tissues for estrogens in women. Estrogens also target the gastrointestinal tract, thymus, pituitary, blood vessels and other tissues. Courtesy of the National Cancer Institute.
Passwater: What are estrogen receptors and how many types are there?
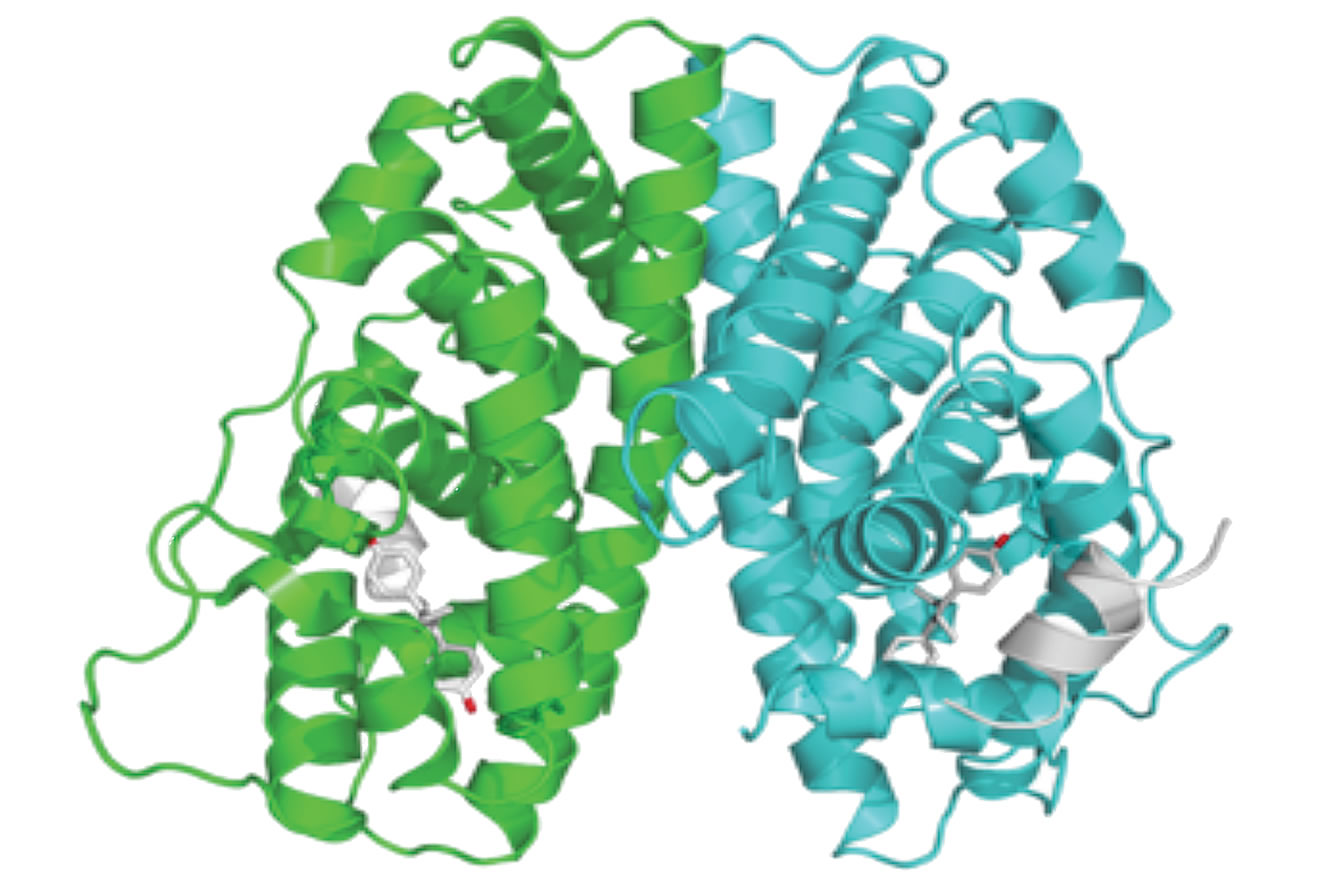
Ritchie: Estrogen receptors are a group of proteins found within cells and on the surface of cells (see Figure 3). They are receptors, hence their name, that respond to estrogen binding. When an estrogen hormone (i.e., estradiol) binds to an estrogen receptor, it activates the receptor and triggers a response within the cell.
Passwater: How do estrogen receptors work?
{kind=link}
Figure 3: Depiction of an alpha-estrogen receptor to illustrate that it is a long protein that folds in such a manner as to attract and hold molecules of estrogens.
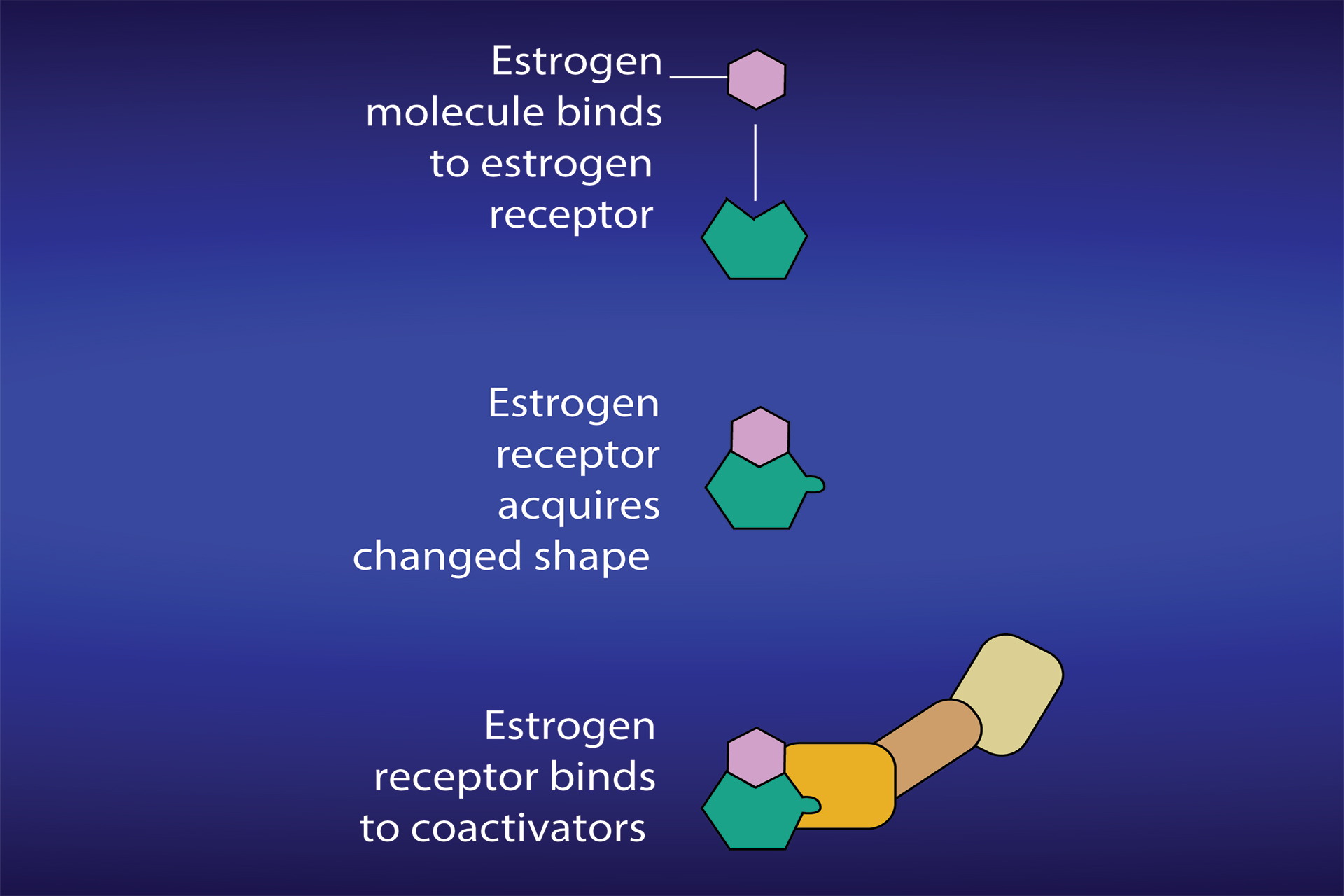
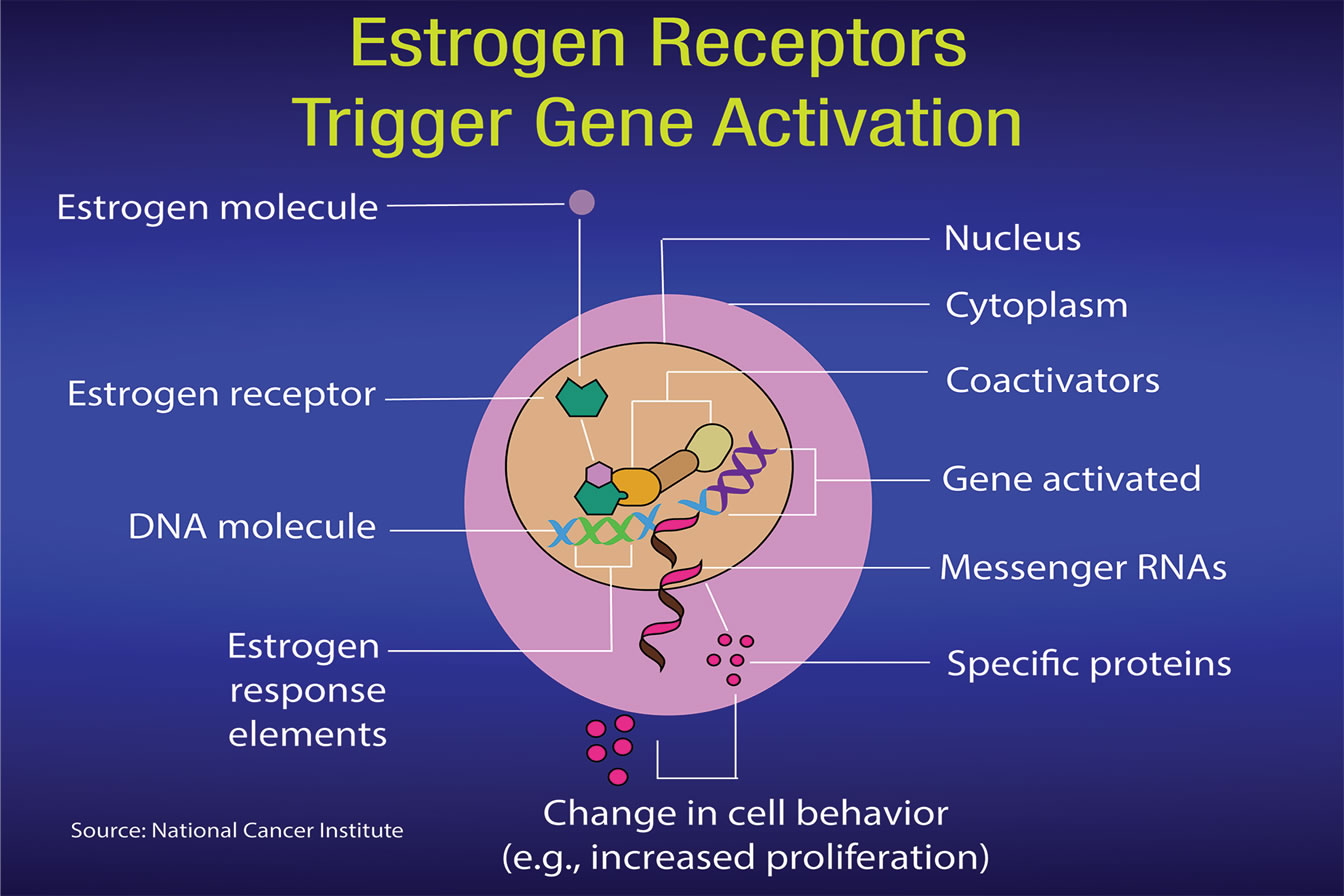
Ritchie: When estrogen binds to the estrogen receptor in the nucleus of a cell, it affects genes involved in development. This, in turn, can form part of an activation signal that will stimulate normal growth or proliferation. The science illustrators at the U. S. National Cancer Institute have drawn figures to help us understand estrogens, estrogen receptors and SERMs (Figures 4a and 4b). The sidebar on p. 54 gives a more detailed explanation for researchers.
Passwater: Back to the basics again. Genes provide the blueprints for making proteins in cells. Each gene makes a specific protein. A gene can be active or dormant. When a chemical activates a gene, it is said to be “upregulated” and it stimulates the production of its protein. Do estrogen receptors work the same in different tissues?
{kind=link}
Figure 4a: Once an estrogen docks within an estrogen receptor, it induces changes in the receptor. Courtesy of National Cancer Institute.
Ritchie: There are two main types of estrogen receptors, namely estrogen receptor alpha (ER-alpha) and estrogen receptor beta (ER-beta).
ER-alpha (ER-α) and ER-beta (ER-β) are found in different proportions in different tissues. ER-α is found in endometrium, breast cancer cells, ovarian stromal cells, and the hypothalamus in females. In males, ER-α is found in the epithelium of the efferent ducts within the male reproductive system. ER-β has been reported as being
{kind=link}
Figure 4b: The changes within the estrogen receptor activate genes that initiate specific proteins. Courtesy of National Cancer Institute
present in ovarian granulosa cells, kidney, brain, bone, heart, lungs, intestinal mucosa, prostate, and endothelial cells. The receptors are sites on which estrogens can bind and stimulate a response within the cell. The response will depend on the location of the cell (i.e., in which tissue it is present) (see Figure 5).
Passwater: Discovery of the ER-β by Professor Jan-Ǻke Gustafsson in 1996 while he was at the Karolinska Institute in Sweden dramatically changed our understanding of how estrogens and phytoestrogens work in the body (4).
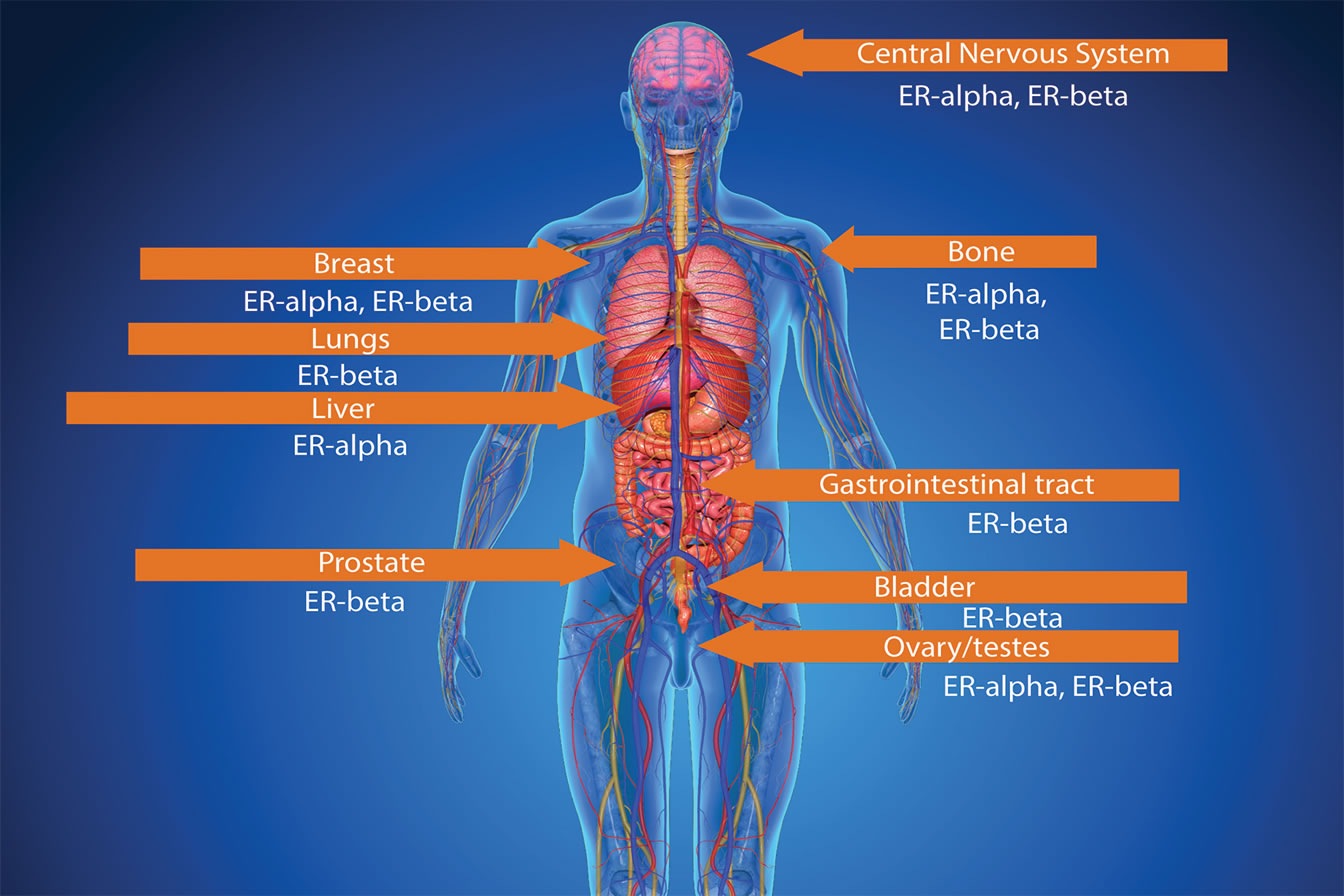{kind=link}
Figure 5: Different tissues contain different amounts of the alpha-estrogen receptor (ER-α) and beta-estrogen receptor. Courtesy of E. Roell/National Cancer Institute.
He is now at the University of Houston. One of the most significant differences between ER-α and ER-β is that ER-α enhances cell division and cell proliferation, a recurring phenomenon in cancer cells. Studies have shown that ER-α is involved in cancer in the uterus and breast, and that the receptor may cause many other negative effects. ER-β, however, is anti-proliferative (5, 6). The estrogen receptors, ER-α and ER-β, oppose and balance one another. While ER-α directs cellular proliferation, ER-β directs cellular differentiation and apoptosis (i.e., programmed destruction of unwanted cells) (7). ER-β is anti-proliferative, in many ways antagonizing ER-α function. Furthermore, phytoestrogens have a binding-preference for ER-β and several epidemiological (correlation) studies indicate a breast cancer preventing effect of this class of compounds (8).
Ritchie: Yes, ER-β may promote anti-proliferative effects. As a result, it may oppose the actions of ER-α in reproductive tissue. This may be useful as some studies have shown that ER-α promotes the growth and proliferation of breast cancer cells. ER-β may also have an important role in the adaptive function of the lung during pregnancy.
ER-β has been reported to be a potent tumor suppressor and as a result it may play an important role in several forms of cancer including prostate cancer. While based at St. Andrews University I was involved with the largest prostate cancer study in Europe in collaboration with the University of Edinburgh where we investigated the effect of phytoestrogens on the risk of prostate cancer.
Passwater: Whoa! May I interrupt you? Perhaps I shouldn’t divert you from the main topic, but a study of phytoestrogens on prostate cancer would be extremely important. Please tell us more about the study.
Ritchie: At the time, this was the largest population-based case-control study of diet, inherited susceptibility and prostate cancer in Europe (9, 10). The study was designed to investigate the effect of phytoestrogen intake and serum concentrations of phytoestrogens on the risk of prostate cancer in men aged 50–74 years. Over 800 cases and controls completed the study and the results showed a significant reduction in the risk of prostate cancer with increasing serum concentrations of enterolactone (i.e., a phytoestrogen from lignans). There was also a significant inverse correlation between the intake of soy foods and the risk of prostate cancer. Overall, the study supported our initial hypothesis that soy foods and enterolactone protect against prostate cancer in older men.
Estrogen Receptors: Detailed Description for Researchers
Estrogen mediates these activities via binding to a specific nuclear receptor protein, the estrogen receptor (ER), which is encoded by two genes (ER-α and ER-β) that function as transcription factors to regulate the expression of target genes. On ligand binding, ER undergoes conformational changes and dissociates from the inactive ER-hsp90 complex. The activated ER enters the nucleus as a homodimer or heterodimer, then binds to a specific DNA sequence, the estrogen response element (ERE), and stimulates estrogen-target gene expression. The two ERs have unique tissue distributions and their own sets of specific functions.
Passwater: Very interesting, indeed! It was worth interrupting you, but let’s get back to your discussion of the differences between the alpha and beta estrogen receptors. You were explaining how the same estrogen—the same identical compound—can produce different results in different tissues due to the differences in the estrogen receptors in the tissues. It’s not so much the estrogen, but the receptor that is most important. The receptor doesn’t work without the estrogen, but what it does depends on is the type of receptor. Do the estrogen receptors result in different proteins in different tissues or organs?
Ritchie: May I be a little technical for a moment?
Passwater: Absolutely! Please do. Some of our readers will appreciate the additional information, while others don’t need any more details than we have already discussed. They can skip ahead to my next question.
Ritchie: OK, I will provide some background here as this may help explain why different proteins result in different tissues. ER-α and ER-β are encoded by distinct genes located on different chromosomes and they have different biological functions. Interestingly, estrogen receptors form dimers (i.e., larger molecules that are made up of both proteins covalently bound together). As a result, the receptors may be made up of ER-α (αα) or ER-β (ββ) homodimers or ERαβ (αβ) heterodimers, which are coexpressed in a number of tissues. In addition, there have been at least three ER-α and five ER-β isoforms identified, which shows the complexity associated with this area of research and why further research is warranted. Both ER-α and ER-β exhibit tissue- and cell-type specific expression and although ER-α and ER-β have overlapping roles, they also have unique roles in estrogen-dependent action within living systems. It has been reported that when both ER-α and ER-β are coexpressed, ER-β exhibits an inhibitory action on ER-α mediated gene expression and, in many instances, opposes the actions of ER-α.
What is significant is the process during which the estrogen binds to the receptor and results in the production of specific proteins. After attachment to estrogen response elements in DNA, the estrogen-receptor complex binds to coactivator proteins causing genes nearby to be activated. The active genes produce molecules of messenger ribonucleic acid (RNA), which guide the synthesis of specific proteins. These proteins can then influence cell behavior in different ways, depending on the cell type involved. In mammary cells, the significance can be cell proliferation, increased cell division, disruption of the cell cycle and checks that take place during cell replication, apoptosis and control of cell death, regulation of cell function, DNA repair and tumor formation.
Interestingly estrogen receptors are over-expressed in around 70% of breast cancers. Different versions of the estrogen response gene have been associated with different risks of developing breast cancer. In tissues with estrogen receptors, the estrogen-responsive genes present and the protein produced may influence the risk and type of cancer.
Passwater: There are various types of phytoestrogens. What are the main types?
Ritchie: Currently more than 300 estrogenic compounds have been identified in plants, the most common of which are isoflavones and coumestans. Lignans have recently been included as phytoestrogens and some flavonoids such as several chalcones, flavanones, flavones and flavonols have also been shown to have estrogenic activity. Herbs such as soy, licorice, red clover, thyme, turmeric, hops, verbena, oregano and damiana are also sources of estrogenic compounds.
Isoflavones occur mainly in one subfamily of Leguminosae, namely the Papilionoidae, although they have been reported occasionally in Compositae and Rosaceae. They were formed about 120 million years ago via the flavone biosynthetic pathway.
Isoflavones were the principal flavonoid compounds necessary for providing antifungal, antibacterial and antiviral protection to plants. Several of these compounds were also potent insecticides with the capacity to mimic estrogen in mammals. Isoflavones constitute the largest proportion of the phenolic antibiotic phytoalexins, compounds that are synthesized only when an infection has started. Isoflavones are closely related to flavones in structure and have similar spectral and chemical properties. The most commonly occurring isoflavones in the diet are genistein and daidzein.
Passwater: Some phytoestrogens are called Selective Estrogen Receptor Modulators? What are SERMs?
Ritchie: SERMS are chemicals that bind to the estrogen receptor in cells in the way that (endogenous) natural estrogen would bind. Once bound, they may cause a conformational change in the receptor similar to that of an antiestrogen binding. In addition, by binding to the estrogen receptor and preventing endogenous estrogen binding (and promoting an estrogenic response), SERMS can block estrogen binding to the binding site and therefore prevent an estrogenic response. In other words, the cell does not receive the stimulus from estrogen to grow and multiply (see Figure 6).
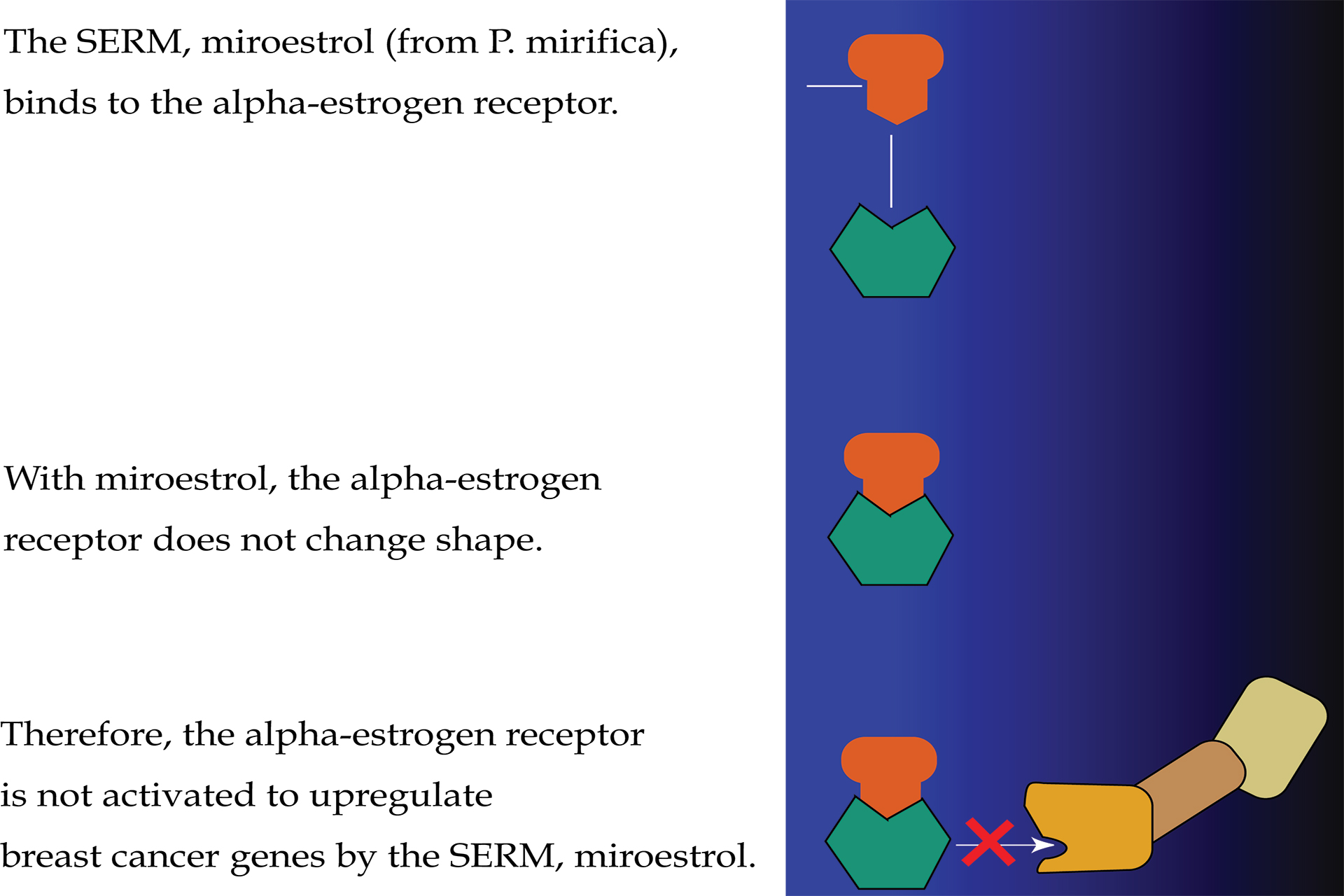{kind=link}
Figure 6: A Selective estrogen receptor modulator (SERM) can act as an anti-estrogen in some estrogen receptors and also as an estrogen in other estrogen receptors. Here, the SERM, miroestrol, is shown as blocking the activation of an alpha-estrogen receptor (ER-α) in a breast cancer cell. Courtesy of the National Cancer Institute.
Passwater: How can a SERM be “selective?”
Ritchie: SERMs are “selective” in that they can block estrogen’s action in breast cells and yet can activate estrogen’s action in other cells, such as bone, liver and uterine cells (see Figure 7).
Cells in other tissues in the body, such as bones and the uterus, also have estrogen receptors. Each estrogen receptor has a slightly different structure, depending on the kind of cell in which it is located. So breast cell estrogen receptors are different from bone cell estrogen receptors and both of those estrogen receptors are different from uterine estrogen receptors.
Passwater: Are all phytoestrogens SERMs?
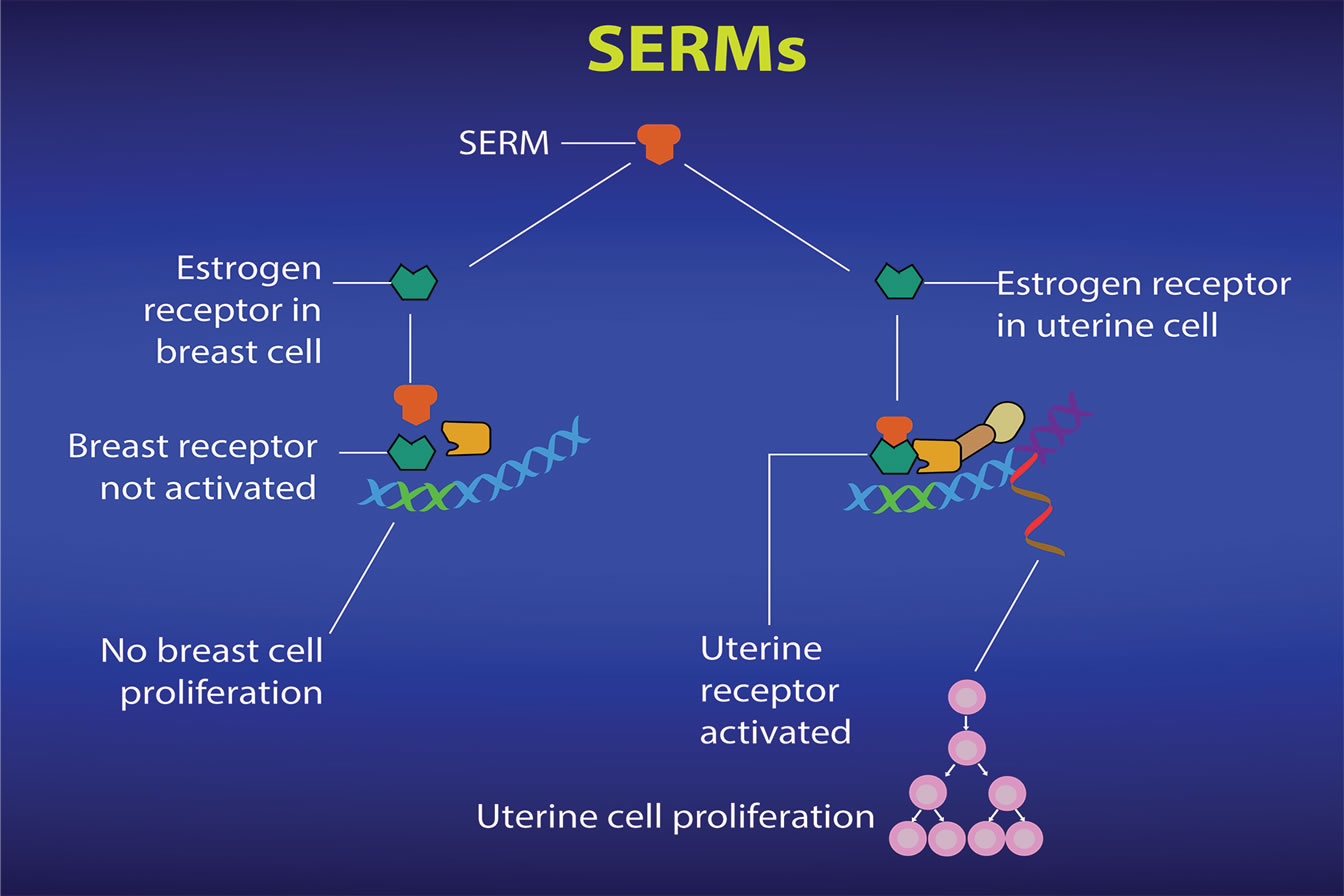{kind=link}
Figure 7: Selective estrogen receptor modulators (SERMs) can produce different responses in different tissues. Courtesy of National Cancer Institute.
Ritchie: Although there are over 300 compounds that have already been identified as phytoestrogens, there are probably more plant-based chemicals that have yet to be discovered and classed as phytoestrogens. As a result, the potential properties and actions of phytoestrogens are based on current research and published literature. SERMs are non-steroidal agents that bind to the estrogen receptor and promote or prevent a partial estrogenic response. Phytoestrogens are so called as they are plant based compounds that can bind to the estrogen receptor and stimulate an estrogenic response. As several phytoestrogens have undergone research and been shown to demonstrate SERM-like properties it can be assumed that, based on current research findings, most phytoestrogens may behave in a similar way to SERMs. That said, a significant amount of research regarding SERM activity has been carried out using specific isoflavones, lignans, coumestans and stilbenes and the assumption about SERM activity is based on these findings.
Passwater: What are estrogen mimics or estrogen disruptive pollutants and how do they differ from phytoestrogens and SERMs? Can phytoestrogens and SERMs protect from estrogen mimics?
Ritchie: Estrogen mimics or endocrine disruptive pollutants may be described as endocrine disruptors. Such agents may consist of drugs, pesticides, compounds used in the plastics industry and in consumer products, industrial byproducts and pollutants, and even some naturally produced botanical chemicals.
There is some evidence that endocrine disruptors may affect humans and wildlife. The effect on humans could be on reproduction, breast development and cancer, prostate cancer and the response of the brain to hormones. Additional effects on the brain, thyroid, metabolism linked to obesity, and the cardiovascular system have also been proposed. Interestingly, the period that is most critical during development is the transition from a fertilized egg into a fully formed infant. As cells begin to grow and differentiate, balancing the effects of hormones and protein changes is very important. As a consequence, exposure to disrupting chemicals may cause considerable damage to a developing fetus. However due to body weight, the same level of exposure to an adult may have no significant effect.
As phytoestrogens may be able to bind to the estrogen receptor and potentially prevent the binding or an endocrine disruptor, they may be able to reduce or limit the effects of endocrine disruptors. As far as I am aware, there is a dearth of studies reporting a negative impact of high phytoestrogen intake (in mothers) on children.
Passwater: Are phytoestrogens safe?
Ritchie: As with all nutrient and non-nutrient components of a diet, it is important to follow a lifestyle and dietary regime that is balanced. To date, I am not aware of any studies in which exposure to phytoestrogens in humans has caused deleterious health effects. Patients with thyroid problems should consult a health care professional if they wish to increase their intake of specific phytoestrogens.
Passwater: Have you found that P. mirifica affects the alpha-estrogen receptor and beta-estrogen receptor differently? If so, what is the significance?
Ritchie: There is some evidence to show that exposure to P. mirifica may alter the level of expression of both receptors by increasing expression of the beta-estrogen receptor relative to the alpha-estrogen receptor. This finding is based on studies involving cell lines. These findings indicated the significance of the period of time over which exposure took place and the P. mirifica concentration to which cells were exposed.
Passwater: You and your colleagues were researching the effect of P. mirifica on estrogen receptors while I was visiting your lab in 2008. What were your findings?
{kind=link}
Richard Passwater, Ph.D., visiting the laboratory of Professor Margaret Ritchie, Ph.D., (right) at Edinburgh Napier University in Edinburgh, Scotland in 2008. Principal researchers included Dr. Michelle Scott (left) and Professor Janis MacCallum.
Ritchie: The findings provided evidence that breast cancer cells (MCF-7 cell line was used) responded to P. mirifica treatment. Two effects were reported: first, the growth of the cells over time and during exposure to varying concentrations of Pueraria mirifica. Another effect that was investigated involved the expression of ER-β relative to ER-α.
The results provided some initial evidence that exposure of breast cancer cells to P. mirifica may increase the ratio of the beta-estrogen receptor relative to the alpha-estrogen receptor over a period of 24 hours and that at higher concentrations, P. mirifica had an anti-proliferative effect on breast cancer cells (11, 12).
Passwater: What is the significance of your findings?
Ritchie: The significance of these studies is that the results were dependent on time and on the concentration of P. mirifica used. It is important to extrapolate the results with care, as in animal and human models, complex physiological processes need to be taken into account when considering the effect on humans.
However, if the expression of the beta-estrogen receptor becomes more prevalent and the ratio of the beta-estrogen receptor relative to the alpha-estrogen receptor is increasing, this might be important because the over-expression of the beta-estrogen receptor has been shown to decrease the transcriptional activation of the alpha-estrogen receptor.
Furthermore, as the beta-estrogen receptor may have anti-proliferative effects and oppose the actions of the alpha-estrogen receptor in reproductive tissue, this may be an important finding on which to base future studies in cancer and breast health.
A feature of research in phytoestrogens (and nutrition in general) has been that duration of exposure and also the quantity used or amount of exposure by an individual seemed to be an important factor in health promotion or disease prevention.
Passwater: Have other researchers followed up on your findings?
Ritchie: An animal study that was carried out and published at the same time reported similar findings. Rats were exposed to increasing levels of P. mirifica over a period of four weeks and similar effects were noted in the ratio of the beta-estrogen receptor to the alpha-estrogen receptor.
Passwater: Where is your research leading you now?
Ritchie: I have been investigating the impact of plant-based products on the immune response and inflammation in human studies while maintaining my interest in phytoestrogen research and nutrition. An ideal study would be to link phytoestrogens with a further study involving the immunological response and investigate the combined effect in humans.
Passwater: Thank you for your very informative discussions, Professor Ritchie. WF
{kind=link}
Dr. Richard Passwater is the author of more than 45 books and 500 articles on nutrition. Dr. Passwater has been WholeFoods Magazine’s science editor and author of this column since 1984. More information is available on his Web site, www.drpasswater.com.
References
1. R.A. Passwater, “Menopause and Pueraria mirifica,” WholeFoods Magazine (October 2016), www.wholefoodsmagazine.com/category/
columns/vitamin-connection.
2. R.A. Passwater, “Pueraria mirifica: Just for Menopause or the Herb of the Decade? Part 1. An Interview with Dr. Garry Gordon,” WholeFoods Magazine (Feb 2007), www.drpasswater.com/nutrition_library/gordon_1.htm.
3. R.A. Passwater, “Pueraria mirifica: Just for Menopause or the Herb of the Decade?: Part 2. An Interview with Dr. Garry Gordon,” WholeFoods Magazine (March 2007), www.drpasswater.com
/nutrition_library/gordon_2(1).htm.
4. G.G. Kuiper, et al., “Cloning of a Novel Receptor Expressed in Rat Prostate and Ovary,” Proc. Natl. Acad. Sci. USA, 93 (12), 5925–5930 (2006).
5. A.M. Brzozowski, et al., “Molecular Basis Of Agonism And Antagonism In The Oestrogen Receptor,” Nature, 389 (6652), 753-758 (1997).
6. O. Treeck, et al., “Estrogen Receptor Beta Exerts Growth-Inhibitory Effects On Human Mammary Epithelial Cells,” Breast Cancer Research and Treatment, 120 (3), 557–565 (2009).
6. A. Morani, M. Warner and J.A. Gustafsson, “Biological Functions And Clinical Implications Of Oestrogen Receptors Alpha And Beta In Epithelial Tissues,” J. Intern. Med. 264 (2), 128-142 (2008).
7. J. Hartman, A. Ström and J.A. Gustafsson, “Estrogen Receptor Beta In Breast Cancer—Diagnostic And Therapeutic Implications,” Steroids 74 (8), 635–641 (2009).
8. C.L. Heald et al., “Phyto-Oestrogens And Risk Of Prostate Cancer In Scottish Men,” Br. J. Nutr. 98(2), 388–396 (2007).
9. C.L. Heald et al., “Phyto-oestrogen Intake In Scottish Men: Use Of Serum To Validate A Self-Administered Food-Frequency Questionnaire In Older Men,” Eur. J. Clin. Nutr. 60 (1), 129–135 (2006).
10. C. Boonchird, T. Mahapanichkul and W. Cherdshewasart, “Differential Binding with ER-alpha and ER-beta of the Phytoestrogen-Rich Plant Pueraria mirifica,” Braz. J. Med. Biol. Res. 43 (2), 195–200 (2010).
11. S. Ramnarine, J. MacCallum, and M. Ritchie, “Phyto-oestrogens: Do They Have A Role In Breast Cancer Therapy?” Proceedings of the Nutrition Society, 68 (OCE2), Jan 2009 , E93 doi: 10.1017/
S0029665109990462.
Published in WholeFoods Magazine November 2016
Subscribe to:
Posts (Atom)